Get the free froi workers comp
Show details
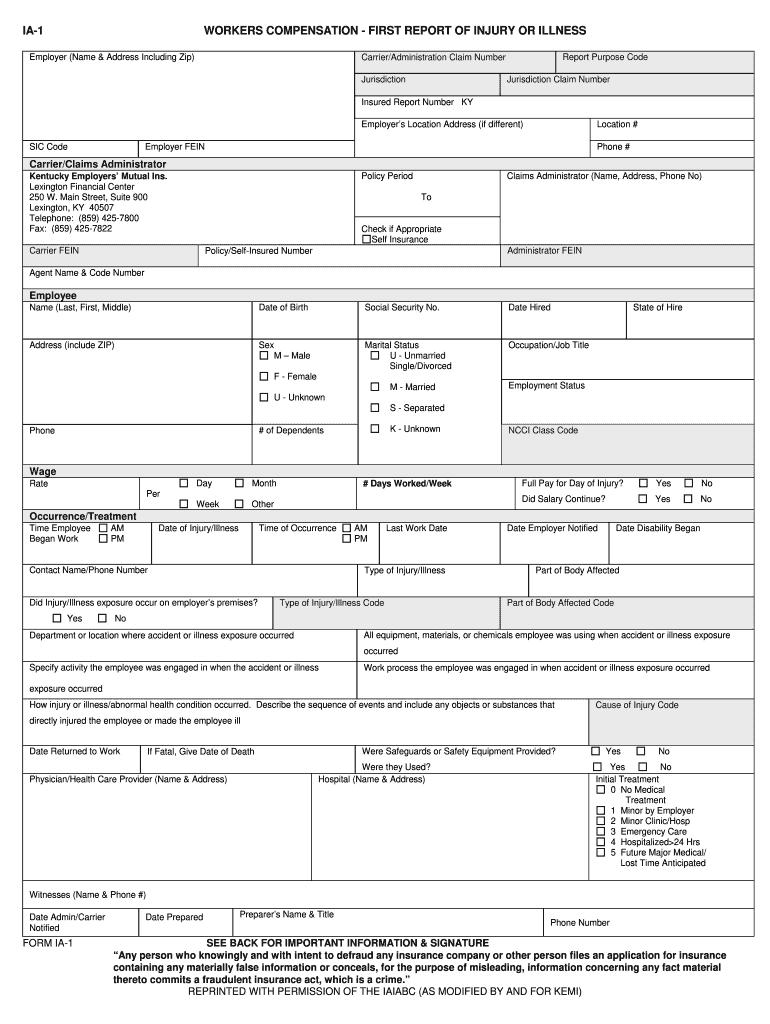
IA-1 WORKERS COMPENSATION - FIRST REPORT OF INJURY OR ILLNESS Employer Name Address Including Zip Report Purpose Code Carrier/Administration Claim Number Jurisdiction Insured Report Number KY Location Employer s Location Address if different SIC Code Employer FEIN Phone Carrier/Claims Administrator Claims Administrator Name Address Phone No Policy Period Kentucky Employers Mutual Ins. Lexington Financial Center 250 W. Main Street Suite 900 Lexing...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign first report of injury froi form
Edit your first report of injury form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your workers comp declaration page form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing froi online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit workers compensation declaration page form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out first notice of injury form
How to fill out Kentucky first report of:
01
Obtain the necessary form: The Kentucky first report of can be obtained from the Kentucky Department of Workers' Claims website or from the employer's insurance provider.
02
Provide accurate information: Fill out the form with accurate information about the injured employee, including their name, address, and social security number.
03
Describe the incident: Clearly describe the details of the incident that led to the employee's injury, including the date, time, and location of the incident.
04
Provide medical information: Include information about any medical treatment the employee has received for their injury, including the name of the treating physician or medical facility.
05
Report wage information: Include the employee's wage information, including their average weekly wage at the time of the injury.
06
Sign and submit: Once the form is filled out completely, sign it and submit it to the appropriate party as indicated on the form.
Who needs Kentucky first report of:
01
Employers: Employers in Kentucky are required by law to report any work-related injuries or illnesses to the Kentucky Department of Workers' Claims.
02
Insurance providers: Insurance providers need the Kentucky first report of to process workers' compensation claims and determine the appropriate coverage and benefits for the injured employee.
03
Injured employees: Injured employees may also need the Kentucky first report of to ensure that their injury is properly reported and documented for workers' compensation purposes.
Fill
froi form
: Try Risk Free
People Also Ask about workers compensation declaration page example
What is timely filing for workers comp in Kentucky?
Time Limits for Filing KY Workers' Comp Claims Written claims for workers' compensation benefits need to be filed with the Department of Workers' Claims. These claims must be filed within two years of the date of injury or last voluntary payment of disability benefits.
What is the statute of limitations on a workplace injury in Kentucky?
The statute of limitations for Kentucky workers' compensation claims is two years. You must file your claim within two years of either sustaining a work-related injury in an accident or discovering the injury.
How long does an employee have to report an injury in Kentucky?
Requirements for Filing In Kentucky, you must report your workplace injury within three days of it occurring. This is known as the "First Report of Injury" and is typically required for workers' compensation insurance.
What is the first report of injury form for workers comp in Kentucky?
Form 1A-1 First Report of Injury (FROI). As soon as you have been notified of a work-related injury, please fill out this form and submit it to EMPLOYERS. This form must be completed within 10 days from notice of an accident. Fatalities must be reported within 24 hours.
How do I file a workers comp claim in KY?
To file for workers' compensation in Kentucky, you will need to submit an Application for Resolution of a Claim, which will then be reviewed by the Division of Claims Processing. Your application will be assigned to an Administrative Law Judge based on your county of residence.
What must the first report of injury contain?
The Employer's First Report of Injury or Illness provides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I edit workers comp declaration page example from Google Drive?
You can quickly improve your document management and form preparation by integrating pdfFiller with Google Docs so that you can create, edit and sign documents directly from your Google Drive. The add-on enables you to transform your what does a workers comp declaration page look like into a dynamic fillable form that you can manage and eSign from any internet-connected device.
How do I edit first report of injury online?
The editing procedure is simple with pdfFiller. Open your declaration page workers compensation in the editor. You may also add photos, draw arrows and lines, insert sticky notes and text boxes, and more.
Can I create an electronic signature for signing my workers comp dec page in Gmail?
Upload, type, or draw a signature in Gmail with the help of pdfFiller’s add-on. pdfFiller enables you to eSign your employers report of injury form and other documents right in your inbox. Register your account in order to save signed documents and your personal signatures.
What is first report of injury?
The first report of injury is a formal document that outlines the details of an employee's injury that occurred in the workplace. It is typically completed shortly after the incident to ensure all relevant information is recorded promptly.
Who is required to file first report of injury?
The employer is generally required to file the first report of injury, although in some instances, the employee may also be involved in the reporting process.
How to fill out first report of injury?
To fill out the first report of injury, gather all relevant information about the incident, including date, time, and location of the injury, a description of how the injury occurred, details regarding the employee and any witnesses, and the type of injury sustained. Ensure that the form is completed accurately and submitted to the appropriate parties.
What is the purpose of first report of injury?
The purpose of the first report of injury is to document the circumstances of a workplace injury for record-keeping, to comply with legal requirements, and to initiate the claims process for workers' compensation.
What information must be reported on first report of injury?
Essential information to be reported includes the employee's name and contact information, details of the injury (nature and location), time and date of the incident, a description of what happened, and any witnesses to the event.
Fill out your froi workers comp form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Ky Workers Comp is not the form you're looking for?Search for another form here.
Keywords relevant to what is froi
Related to workers comp first report of injury form







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
